ACR20 RESPONSE RATES OVER TIME
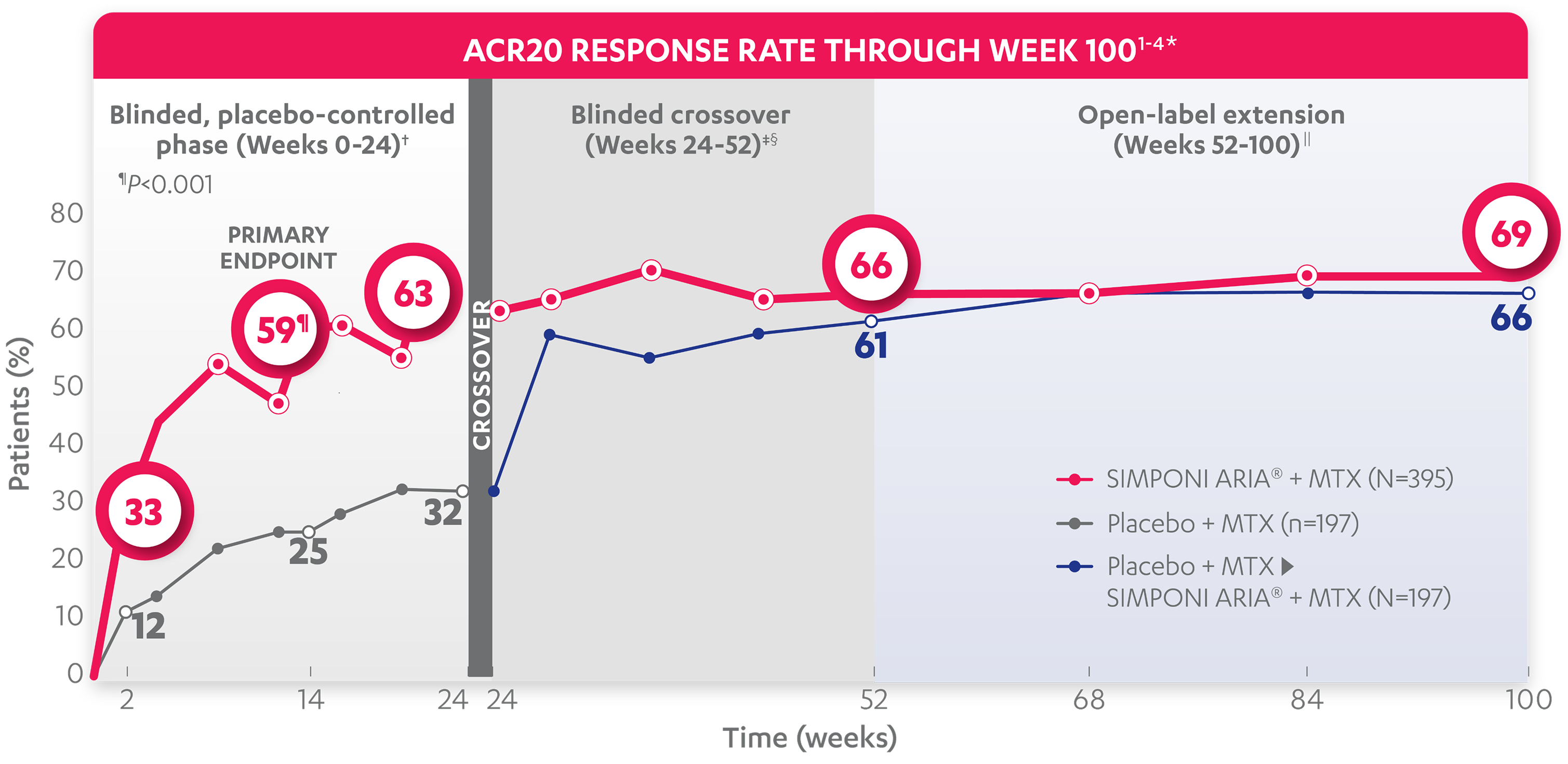
ACR20 RESPONSE RATE THROUGH WEEK 1001-4*
BLINDED, PLACEBO-CONTROLLED PHASE (WEEKS 0-24)†
ACR20 response at Week 14 (primary endpoint):
of patients receiving
SIMPONI ARIA® + MTX (231/395)
achieved ACR20 response (P<0.001)
of patients receiving placebo +
MTX (49/197)1-3
Rapid ACR20 response at Week 2:
of patients receiving
SIMPONI ARIA® + MTX (131/395)
achieved ACR20 response
of patients receiving placebo +
MTX (23/197)1-3
ACR20 response at Week 24:
of patients receiving
SIMPONI ARIA® + MTX (248/395)
achieved ACR20 response
of patients receiving placebo +
MTX (63/197)1-3
ACR20 responses at Week 2 and Week 24 were not adjusted for multiplicity. Therefore, statistical significance has not been established.
WEEK 24 CROSSOVER‡§
ACR20 response at Week 52‡§:
of patients receiving SIMPONI ARIA® + MTX (n=395) achieved ACR20 response
of patients receiving placebo who crossed over to SIMPONI ARIA® + MTX at Week 24 (n=197)2
OPEN-LABEL EXTENSION||
ACR20 response through Week 100||:
of patients receiving SIMPONI ARIA® + MTX (n=395) achieved ACR20 response
of patients receiving placebo who crossed over to SIMPONI ARIA® + MTX at Week 24 (n=197)4
ACR20 responses at Week 2 and Week 24 were not adjusted for multiplicity. Therefore, statistical significance has not been established.
Study design: GO-FURTHER™ was a global, multicenter, randomized, double-blind, placebo-controlled study in 592 adult patients who had moderately to severely active RA despite a stable dose of MTX (15-25 mg/week) for ≥3 months and who had not been previously treated with an anti-TNF agent. Moderately to severely active RA was defined as ≥6 swollen joints (out of 66 total) and ≥6 tender joints (out of 68 total), RF positive and/or anti-CCP antibody positive, and CRP ≥1.0 mg/dL. Patients were randomized to receive SIMPONI ARIA® 2 mg/kg + MTX (n=395) or placebo + MTX (n=197) as a 30-minute IV infusion at Weeks 0 and 4, and then q8w through Week 100. At Week 16, patients in the placebo + MTX group with <10% improvement from baseline in both swollen joint count and tender joint count began receiving SIMPONI ARIA® 2 mg/kg beginning with an induction regimen at Weeks 16 and 20, followed by maintenance infusions q8w in a blinded manner. At Week 24, all patients remaining in the placebo + MTX group began receiving SIMPONI ARIA® 2 mg/kg beginning with an induction regimen at Weeks 24 and 28, followed by maintenance infusions q8w in a blinded manner. All patients continued to receive MTX. The primary endpoint was the percentage of patients achieving an ACR20 response at Week 14.2
ACR20=20% improvement in American College of Rheumatology criteria; ACR50=50% improvement in American College of Rheumatology criteria; ACR70=70% improvement in American College of Rheumatology criteria; CCP=cyclic citrullinated peptide; CRP=C‑reactive protein; DMARD=disease-modifying anti-rheumatic drug; ITT=intention-to-treat; IV=intravenous; MTX=methotrexate; q8w=every 8 weeks; RA=rheumatoid arthritis; RF=rheumatoid factor; TNF=tumor necrosis factor.
ACR50 RESPONSE RATES OVER TIME
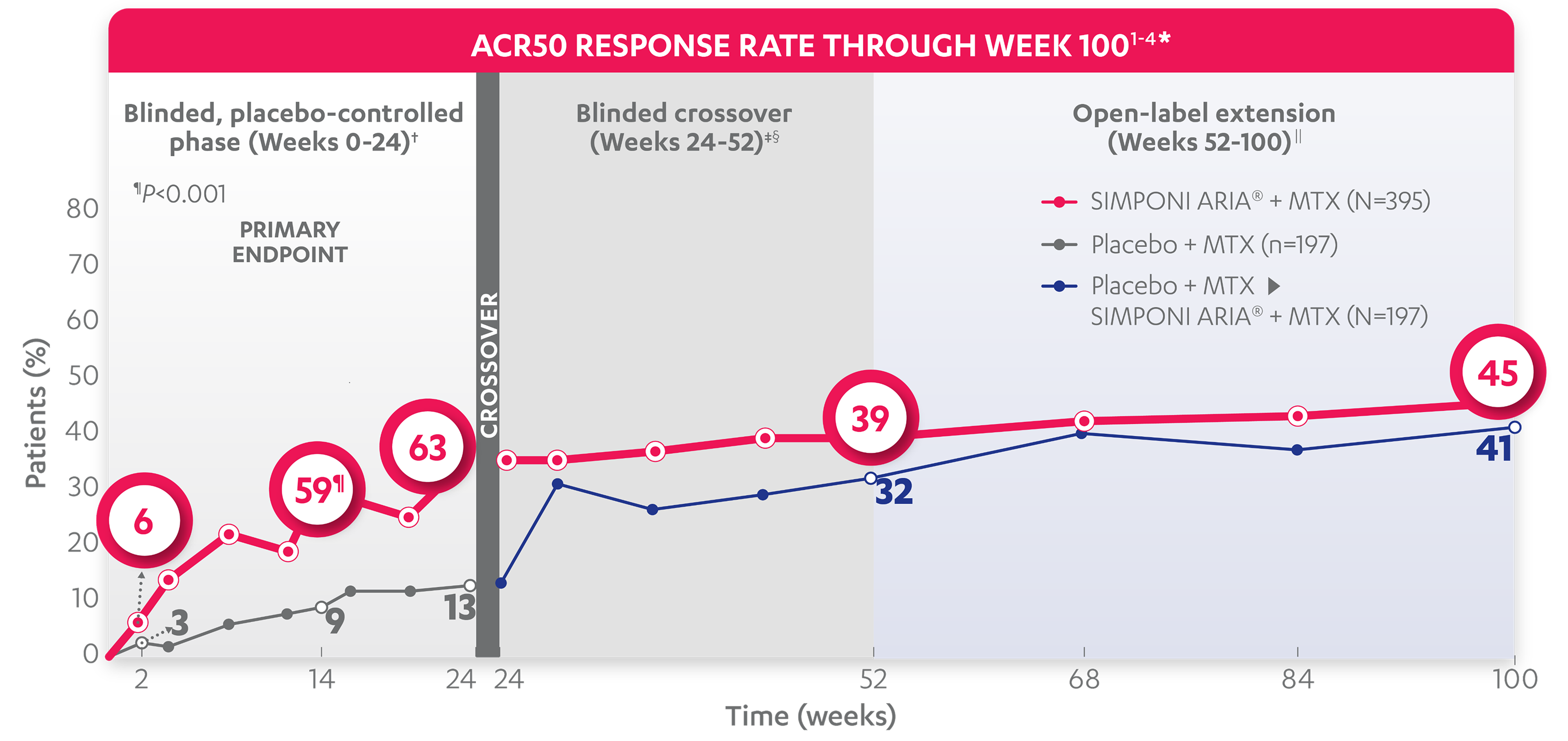
ACR50 RESPONSE RATE THROUGH WEEK 1001-4*
BLINDED, PLACEBO-CONTROLLED PHASE (WEEKS 0-24)†
ACR50 response at Week 14:
of patients receiving
SIMPONI ARIA® + MTX (118/395)
achieved ACR50 response
of patients receiving placebo +
MTX (17/197)1-3
ACR50 response at Week 24:
of patients receiving
SIMPONI ARIA® + MTX (138/395)
achieved ACR50 response
(P<0.001)
of patients receiving placebo +
MTX (26/197)1-3
ACR50 responses at Week 2 and Week 24 were not adjusted for multiplicity. Therefore, statistical significance has not been established.
WEEK 24 CROSSOVER†‡
ACR50 response at Week 52§:
of patients receiving SIMPONI ARIA® + MTX (153/395) achieved ACR50 response
of patients receiving placebo who crossed over to SIMPONI ARIA® + MTX at Week 24 (62/197)2
OPEN-LABEL EXTENSION||
ACR50 response through Week 100||:
of patients receiving SIMPONI ARIA® + MTX (178/395) achieved ACR50 response
of patients receiving placebo who crossed over to SIMPONI ARIA® + MTX at Week 24 (81/197)4
ACR50 responses at Week 2 and Week 14 were not adjusted for multiplicity. Therefore, statistical significance has not been established.
Study design: GO-FURTHER™ was a global, multicenter, randomized, double-blind, placebo-controlled study in 592 adult patients who had moderately to severely active RA despite a stable dose of MTX (15-25 mg/week) for ≥3 months and who had not been previously treated with an anti-TNF agent. Moderately to severely active RA was defined as ≥6 swollen joints (out of 66 total) and ≥6 tender joints (out of 68 total), RF positive and/or anti-CCP antibody positive, and CRP ≥1.0 mg/dL. Patients were randomized to receive SIMPONI ARIA® 2 mg/kg + MTX (n=395) or placebo + MTX (n=197) as a 30-minute IV infusion at Weeks 0 and 4, and then q8w through Week 100. At Week 16, patients in the placebo + MTX group with <10% improvement from baseline in both swollen joint count and tender joint count began receiving SIMPONI ARIA® 2 mg/kg beginning with an induction regimen at Weeks 16 and 20, followed by maintenance infusions q8w in a blinded manner. At Week 24, all patients remaining in the placebo + MTX group began receiving SIMPONI ARIA® 2 mg/kg beginning with an induction regimen at Weeks 24 and 28, followed by maintenance infusions q8w in a blinded manner. All patients continued to receive MTX. The primary endpoint was the percentage of patients achieving an ACR20 response at Week 14.2
ACR20=20% improvement in American College of Rheumatology criteria; ACR50=50% improvement in American College of Rheumatology criteria; ACR70=70% improvement in American College of Rheumatology criteria; CCP=cyclic citrullinated peptide; CRP=C-reactive protein; DMARD=disease-modifying anti-rheumatic drug; ITT=intention-to-treat; IV=intravenous; MTX=methotrexate; q8w=every 8 weeks; RA=rheumatoid arthritis; RF=rheumatoid factor; TNF=tumor necrosis factor.
ACR70 RESPONSE RATES OVER TIME
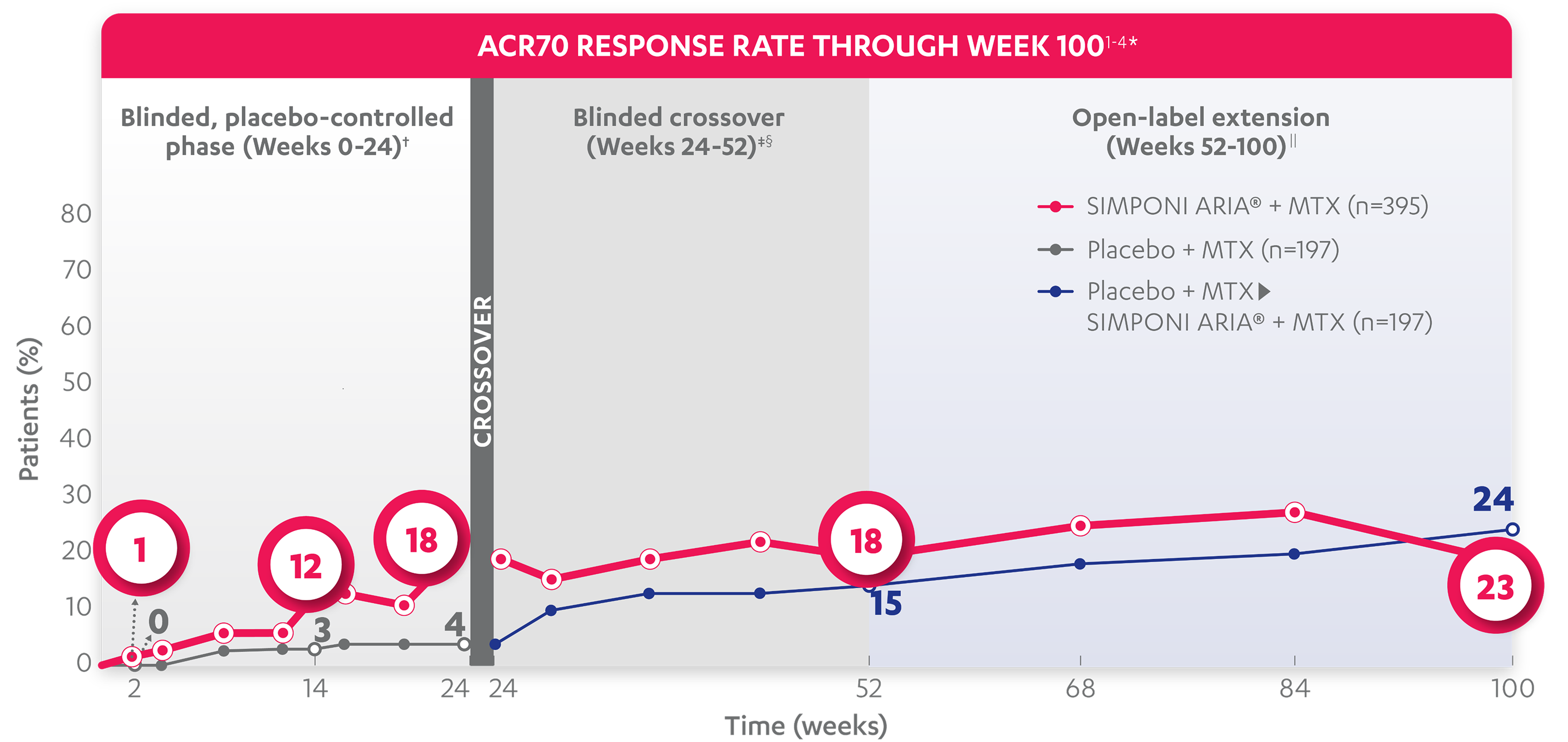
ACR70 RESPONSE RATE THROUGH WEEK 1001-4*
BLINDED, PLACEBO-CONTROLLED PHASE (WEEKS 0-24)†
ACR70 response at Week 14:
of patients receiving
SIMPONI ARIA® + MTX (49/395)
achieved ACR70 response
of patients receiving placebo +
MTX (6/197)1-3
ACR70 response at Week 24:
of patients receiving
SIMPONI ARIA® + MTX (69/395)
achieved ACR70 response
of patients receiving placebo +
MTX (8/197)1-3
ACR70 responses at Week 2 and Week 24 were not adjusted for multiplicity. Therefore, statistical significance has not been established.
WEEK 24 CROSSOVER†‡
ACR70 response through Week 52:
of patients receiving
SIMPONI ARIA® + MTX (n=395)
achieved ACR70 response
of patients receiving placebo who crossed over to SIMPONI ARIA® + MTX at Week 24 (n=197)2
OPEN-LABEL EXTENSION||
ACR70 response through Week 100||:
of patients receiving
SIMPONI ARIA® + MTX (n=395)
achieved ACR70 response
of patients receiving placebo who crossed over to SIMPONI ARIA® + MTX at Week 24 (n=197)4
ACR70 responses at Week 2, Week 14, and Week 24 were not adjusted for multiplicity. Therefore, statistical significance has not been established.
Study design: GO-FURTHER™ was a global, multicenter, randomized, double-blind, placebo-controlled study in 592 adult patients who had moderately to severely active RA despite a stable dose of MTX (15-25 mg/week) for ≥3 months and who had not been previously treated with an anti-TNF agent. Moderately to severely active RA was defined as ≥6 swollen joints (out of 66 total) and ≥6 tender joints (out of 68 total), RF positive and/or anti-CCP antibody positive, and CRP ≥1.0 mg/dL. Patients were randomized to receive SIMPONI ARIA® 2 mg/kg + MTX (n=395) or placebo + MTX (n=197) as a 30-minute IV infusion at Weeks 0 and 4, and then q8w through Week 100. At Week 16, patients in the placebo + MTX group with <10% improvement from baseline in both swollen joint count and tender joint count began receiving SIMPONI ARIA® 2 mg/kg beginning with an induction regimen at Weeks 16 and 20, followed by maintenance infusions q8w in a blinded manner. At Week 24, all patients remaining in the placebo + MTX group began receiving SIMPONI ARIA® 2 mg/kg beginning with an induction regimen at Weeks 24 and 28, followed by maintenance infusions q8w in a blinded manner. All patients continued to receive MTX. The primary endpoint was the percentage of patients achieving an ACR20 response at Week 14.2
ACR20=20% improvement in American College of Rheumatology criteria; ACR50=50% improvement in American College of Rheumatology criteria; ACR70=70% improvement in American College of Rheumatology criteria; CCP=cyclic citrullinated peptide; CRP=C-reactive protein; DMARD=disease-modifying anti-rheumatic drug; ITT=intention-to-treat; IV=intravenous; MTX=methotrexate; PsA=psoriatic arthritis; q8w=every 8 weeks; RA=rheumatoid arthritis; RF=rheumatoid factor; TNF=tumor necrosis factor.